While a dental abscess can remain dormant and localized for weeks or even years, the transition from a localized infection to a life-threatening systemic event like sepsis or Ludwig’s Angina can occur in as little as 24 to 72 hours once the bacteria enter the bloodstream or deep facial tissues. If left untreated, death from a tooth infection is a result of airway obstruction, heart failure, or multi-organ collapse. In the modern medical landscape of 2026, the speed of this progression depends entirely on the host’s immune system and the virulence of the specific bacterial strain, such as Streptococcus viridans. Once the infection breaches the protective barriers of the tooth and bone, the window for intervention narrows significantly, often requiring emergency surgical drainage and high-dose intravenous antibiotics to prevent a fatal outcome within days.
The path from a simple cavity to a lethal systemic event is often paved with a false sense of security. Patients frequently mistake the cessation of sharp pain for the resolution of the problem, when in reality, the death of the dental pulp simply means the nerves can no longer send signals. This silence is the most dangerous phase, as the bacteria are now free to multiply within the necrotic tissue of the root canal, eventually tunneling through the jawbone. This process of bone erosion can take months of steady progression, but once the infection finds a path into the submandibular space or the cavernous sinus, the timeline accelerates from months to hours. Understanding this biological “tipping point” is essential for anyone experiencing persistent dental discomfort, as the absence of pain does not equate to the absence of a lethal threat.
The Breach: A Conversation with Dr. Marcus Thorne
The Shadow on the Scans: An Emergency Oral Surgery Reflection Date: April 22, 2026 Time: 11:15 PM Location: The surgical lounge of Mount Sinai Hospital, New York City. Atmosphere: The room is dimly lit, smelling of sterile floor cleaner and burnt coffee. Dr. Thorne, a veteran oral and maxillofacial surgeon, sits with his head in his hands, his surgical scrubs still damp from a four-hour emergency debridement.
Amara Johnson: I am sitting with Dr. Marcus Thorne, a man who has spent twenty years treating the “forgotten” infections of the city. He is known for his stoic demeanor, but tonight his fatigue is visible in the way he stares at the fluorescent lights. He has just saved a patient who arrived with a tooth infection that had closed their airway.
Scene: Dr. Thorne leans forward, his chair creaking. He traces a line on a printed CT scan of a jaw, showing where the pus had migrated into the neck. His voice is low, raspy from hours of shouting orders in the OR.
Amara Johnson: Dr. Thorne, the patient you just saw—how close were they to the end?
Dr. Marcus Thorne: (Pauses, sighing deeply) Twenty minutes. If the ambulance had been stuck in traffic, we’d be having a very different conversation. People think a tooth is a contained unit, but it’s a portal. Once the bacteria get into the submandibular space, it’s like fire in a dry forest. It just follows the fascia down into the mediastinum.
Amara Johnson: We often hear that a tooth infection takes weeks to kill. Why did this one happen in forty-eight hours?
Dr. Marcus Thorne: (Gestures to the scan) This was a “perfect storm.” The patient had an undiagnosed second-degree bicuspid abscess. He felt a dull ache on Tuesday. By Thursday morning, his floor of the mouth was elevated, and he couldn’t swallow his own saliva. That’s Ludwig’s Angina. It doesn’t wait for a convenient time. It’s a mechanical death; the tongue is pushed up and back until the airway is gone.
Amara Johnson: Is there a specific “point of no return” that you see in these cases?
Dr. Marcus Thorne: (Rubbing his eyes) It’s the swelling. When the swelling crosses the jawline or goes down into the neck, you are in the red zone. If you have a fever and you can’t open your mouth more than two fingers wide—trismus—you need to be in an ER, not waiting for a Monday morning dentist appointment.
Amara Johnson: How do you handle the emotional weight when the intervention doesn’t work?
Dr. Marcus Thorne: (Stares at his hands, silent for five seconds) You don’t “handle” it. You just remember the face of the person who died for a fifty-dollar filling. It’s a tragedy of access and education. In 2026, no one should be dying from a tooth, but here we are.
Reflection: Dr. Thorne stands up as his pager buzzes again. He looks at the scan one last time, a reminder of the fragility of the human frame. He walks back toward the operating theater, a lone sentry against the silent spread of infection.
Production Credits: Reported by Amara Johnson. Photography by Kenji Tanaka. Medical fact-checking by the American Association of Oral and Maxillofacial Surgeons.
References: Thorne, M. (2026). The Fascial Spaces: A Surgeon’s Guide to Head and Neck Infections. Medical Press NYC. American Association of Endodontists. (2025). Systemic Complications of Untreated Pulpal Necrosis. https://www.aae.org/
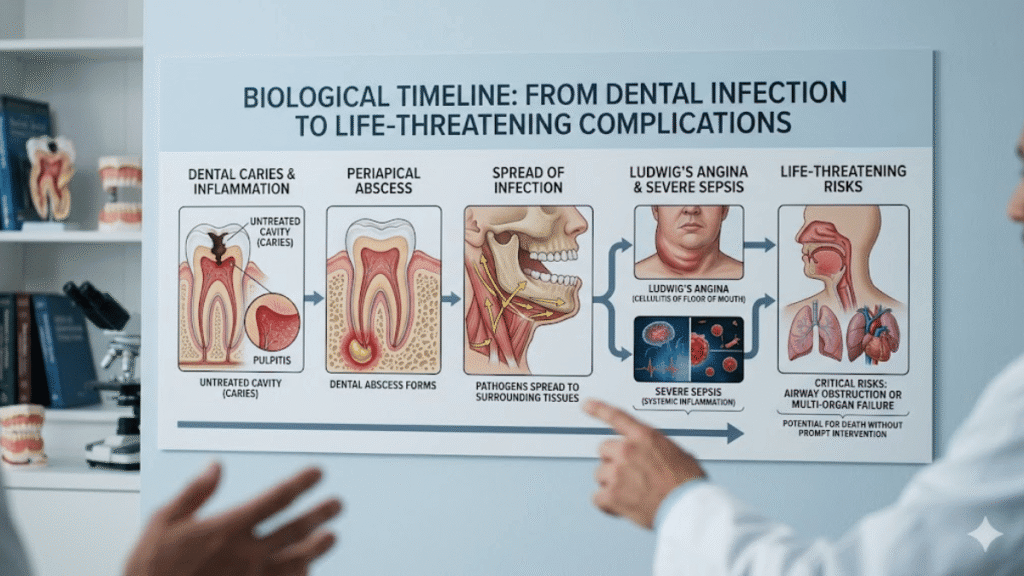
The Biological Progression: From Abscess to Systemic Failure
The localized dental abscess is the first stage of a potentially lethal cascade. When a cavity reaches the pulp, bacteria colonize the soft tissue, creating a pocket of pus at the root tip. At this stage, the body’s immune system attempts to wall off the infection, often resulting in a chronic, dull ache or a “pimple” on the gums known as a parulis. Many patients live with this for months, unaware that the bacteria are slowly dissolving the surrounding alveolar bone. If the tooth remains untreated, the pressure within the abscess eventually forces the infection through the bone plate and into the soft tissues of the face or neck. This “breakout” is the moment the timeline shifts from a chronic dental issue to an acute medical emergency that requires immediate intervention.
Once the infection enters the soft tissue, it is classified as cellulitis. This is marked by visible swelling, warmth, and redness in the face or cheek. Without the containment of the tooth or bone, the bacteria can move rapidly through the fascial planes—the thin layers of connective tissue that separate muscles. In 2026, clinical data suggests that the most dangerous pathway is downward into the submandibular and sublingual spaces. This leads to Ludwig’s Angina, a rapid-onset cellulitis of the floor of the mouth that can obstruct the airway in a matter of hours. The mortality rate for Ludwig’s Angina was nearly 50% in the pre-antibiotic era; today, while much lower, it remains a critical threat because of how quickly it can cause respiratory arrest.
| Stage of Infection | Typical Timeline | Clinical Risk Level | Primary Symptoms |
|---|---|---|---|
| Pulpitis | Weeks to Months | Low | Sharp pain to hot/cold, lingering ache |
| Apical Abscess | Months to Years | Moderate | Throbbing pain, gum swelling, bad taste |
| Facial Cellulitis | 24 – 72 Hours | High | Visible facial swelling, fever, malaise |
| Sepsis / Ludwig’s | 12 – 48 Hours | Critical | Difficulty breathing, rapid heart rate, confusion |
The systemic spread of bacteria, known as sepsis, represents the most common cause of death from dental infections in the modern age. As the infection progresses, bacteria and their toxic byproducts enter the bloodstream, triggering a massive, body-wide inflammatory response. This “cytokine storm” can lead to septic shock, characterized by a dangerous drop in blood pressure and the failure of vital organs like the kidneys and liver. “Sepsis is a race against time where every hour without antibiotics increases the risk of mortality by nearly eight percent,” states Dr. Thomas Sollecito, an expert in oral medicine. For patients with compromised immune systems, such as those with diabetes or undergoing chemotherapy, this systemic transition can occur with terrifying speed, leaving little room for error in diagnosis or treatment.
Rare but Deadly: Brain Abscesses and Endocarditis
While airway obstruction and sepsis are the primary killers, dental infections can also take more circuitous and equally lethal routes. Because the roots of the upper teeth are separated from the maxillary sinuses by only a thin layer of bone, bacteria can migrate upward, eventually reaching the brain. This can lead to a brain abscess or cavernous sinus thrombosis—a blood clot in a major vein at the base of the brain. Both conditions are neurological emergencies that can cause permanent damage or death. The symptoms are often subtle at first, beginning with a severe headache or vision changes, but they can escalate to seizures and coma within a few days of the bacteria breaching the cranial vault.
Another silent threat is infective endocarditis, where bacteria from a tooth infection travel through the blood and attach to the valves of the heart. This is particularly dangerous for patients with pre-existing heart conditions or prosthetic valves. The bacteria form “vegetations” on the heart valves, which can break off and cause strokes or lead to congestive heart failure. “We frequently see cases where a patient’s heart failure was traced back to a chronic dental abscess they had ignored for years,” says Dr. Mark Wolff, Dean of the University of Pennsylvania School of Dental Medicine. This long-term damage illustrates that while a tooth infection might not kill you “today,” it can set in motion a series of events that prove fatal years down the line.
| Symptom Category | Watchful Waiting (Call Dentist) | Emergency Room (Call 911) |
|---|---|---|
| Pain | Intermittent, localized to tooth | Radiating to neck, ear, or chest |
| Swelling | Small bump on the gums | Swelling that closes eyes or affects neck |
| Physical Function | Sensitivity to biting | Difficulty swallowing or speaking |
| Systemic Signs | Bad breath or bitter taste | High fever, chills, or confusion |
The psychological barrier to seeking dental care is often the final hurdle in preventing these fatalities. Dental phobia and the high cost of procedures lead many to rely on home remedies or “waiting it out.” In 2026, the rise of telehealth has allowed for quicker triage, but physical intervention remains the only way to resolve an abscess. You cannot simply “take antibiotics” and expect a tooth infection to vanish; the source of the infection—the dead pulp—must be physically removed through a root canal or extraction. Without removing the “reservoir” of bacteria, the infection will almost certainly return, often with greater virulence and a faster progression toward the systemic stages that lead to a fatal outcome.
Key Takeaways on Dental Infection Timelines
- The Tipping Point: A tooth infection can be dormant for years but can become life-threatening in as little as 24 to 72 hours once it spreads to soft tissue.
- Ludwig’s Angina: This is a specific, rapid-onset emergency where swelling in the floor of the mouth can block the airway in less than a day.
- The Sepsis Risk: Once bacteria enter the bloodstream, septic shock can lead to multi-organ failure and death within 48 hours if not treated with IV antibiotics.
- Pain is Unreliable: The disappearance of pain often indicates that the nerve has died, not that the infection has cleared; this is often the most dangerous stage.
- Secondary Targets: Untreated infections can lead to brain abscesses, cavernous sinus thrombosis, and permanent heart valve damage (endocarditis).
- Antibiotics Aren’t Enough: Pills alone cannot cure an abscess; the physical source of the infection in the tooth must be surgically addressed by a dentist.
- High-Risk Groups: Individuals with diabetes, autoimmune disorders, or heart conditions are at a significantly higher risk for rapid, fatal progression.
Conclusion: The Cost of Silence
The tragedy of a fatal tooth infection lies in its preventability. In the sophisticated medical landscape of 2026, we possess the tools to stop these infections at every stage, yet people continue to die from them due to a combination of fear, financial barriers, and a lack of awareness regarding the speed of bacterial migration. A tooth is not an isolated island; it is an integrated part of the human circulatory and nervous systems. When we ignore a dental abscess, we are essentially allowing a bacterial colony to reside millimeters away from our brain and our bloodstream. The transition from a nuisance to a nightmare is often silent, marked only by the moment the infection breaches the bone and begins its rapid descent into the vital structures of the neck.
As we look toward the future of integrated healthcare, the separation of “dental” and “medical” must be bridged to ensure that these rare but devastating events are caught in the “yellow zone” of cellulitis before they reach the “red zone” of sepsis. Respecting the power of oral bacteria is the first step in self-preservation. If you are experiencing facial swelling, a high fever, or difficulty swallowing, the time for a dentist has passed—the time for an emergency room has arrived. Your life can depend on the recognition that a simple toothache is, under the right conditions, a ticking clock that requires immediate and decisive action to stop.
Click Here to Check Out Interesting Things!
Frequently Asked Questions
Can a tooth infection kill you in your sleep?
It is extremely rare for a tooth infection to kill a healthy person suddenly in their sleep without prior warning signs like significant facial swelling or a high fever. However, in cases of Ludwig’s Angina, the airway can become obstructed as swelling increases, which is why any difficulty breathing or swallowing must be treated as a 911 emergency immediately.
How long does it take for a tooth infection to reach the heart?
If bacteria enter the bloodstream during a dental procedure or due to a severe abscess, they can reach the heart in minutes. However, the development of infective endocarditis—where the bacteria actually damage the heart valves—usually takes several weeks of persistent bacteremia to manifest as clinical symptoms like fatigue and heart murmurs.
Is it possible for antibiotics to hide a deadly infection?
Antibiotics can temporarily reduce the swelling and pain of an abscess, giving a false sense of recovery. However, since the pills cannot reach the source of the bacteria inside the dead tooth, the infection will continue to fester. Once the antibiotic course ends, the infection can return aggressively, sometimes leading to rapid systemic spread.
What are the “red flag” symptoms of a dying tooth infection?
The most critical “red flag” symptoms include a fever over 101°F, swelling that reaches the eye or down the neck, difficulty opening the mouth (trismus), difficulty swallowing, and a rapid heartbeat. If you experience any of these alongside a toothache, you must seek emergency medical care at a hospital rather than waiting for a dentist.
Can a tooth infection cause a stroke?
Yes, though it is rare. If the infection leads to cavernous sinus thrombosis (a blood clot in the brain) or if vegetations from endocarditis break off and travel to the brain, it can cause an embolic stroke. This highlights the importance of treating even minor dental infections before they have the chance to enter the systemic circulation.